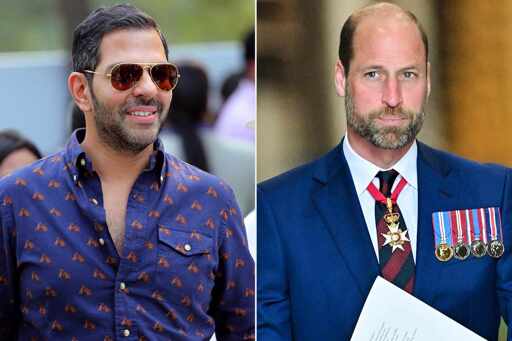
Sunjay Kapur, friend of Prince William and ex-husband of Bollywood star Karisma Kapoor, reportedly died of anaphylactic shock after being stung by a bee during a polo match in Windsor, England.
Airway management contains much more than just “getting a hole into the neck” - it starts with nebulised adrenaline (which works wonders but must be used in moderation due to the side effects), regular endotracheal intubation with a (preferably video)laryngoscope, if necessary with a tube that is resistant against swelling(woodbridge tube) before a cricothyrotomy (not a tracheotomy,see below) is performed - and is supported by intravasal drugs (mostly adrenaline, a glucocorticoid and H1 blockers, in some cases also a beta2 antagonist and a anticholinergic agent). A cric is always the last choice due to the high risk to benefit ratio.
Even a qualified responder won’t do a tracheotomy - emergency tracheotomies are extremly rare and basically only necessary when either the pharyngeal structures are damaged beyond rescue (due to trauma, cancer or some real rare diseases. This is not the case in anaphylaxis. The reasons for a tracheotomy not being used are many. It takes a lot of time,is far harder to achieve (getting between the tracheal cartilage is not as easy as it sounds), the risk of “hitting” structures that are vital to the patient are considerable (seen a patient who’s v.jug. ran over the spot) and the required training to do it is considerable - Besides ENTs and sometimes intensivists around here none therefore is even trained to do it anymore. I occasionally teach emergency surgical techniques to interns and med students and we don’t do so,beyond explaining the core concept, neither does any uni in central or northern Europe that I know of, same goes for AU/NZ.
A “cric” is far easier, but still takes some skill - both needle or open surgical cric(I would prefer the later) does require correct identification of the landmarks (which can be tough), good surgical technique and mainly: Training - lots of it. We therefore teach paramedics only a needle based approach (in combination with jet ventilation) - and tbh, most EM docs are not that “up to standard” in this technique as well - even though a cric is far easier than a trach.
The technique mentioned here will, with a 95% chance, not lead to any airway access, damage the thyroid (which bleeds like fuck) or the vagina carotica (the structure that contains the large vessels in the neck as well as the nervus vagus). If that happens the patient is usually beyond rescue. A case that, even if in cardiac arrest, had at least a slim chance of survival, will then certainly die - post anaphylaxis arrests with good bystander CPR have a somewhat improved prognosis - considering that that a laymans trach likely would diminish chest compression quality for minutes this would simply take that chance away from the patient.
Whoever thinks he needs to teach that in civilan responder courses needs to be fired - it’s not part in any curriculum worldwide as they are all more or less based on the same guidelines.


As it came up here a bit of a longer explanation.
Airway management contains much more than just “getting a hole into the neck” - it starts with nebulised adrenaline (which works wonders but must be used in moderation due to the side effects), regular endotracheal intubation with a (preferably video)laryngoscope, if necessary with a tube that is resistant against swelling(woodbridge tube) before a cricothyrotomy (not a tracheotomy,see below) is performed - and is supported by intravasal drugs (mostly adrenaline, a glucocorticoid and H1 blockers, in some cases also a beta2 antagonist and a anticholinergic agent). A cric is always the last choice due to the high risk to benefit ratio.
Even a qualified responder won’t do a tracheotomy - emergency tracheotomies are extremly rare and basically only necessary when either the pharyngeal structures are damaged beyond rescue (due to trauma, cancer or some real rare diseases. This is not the case in anaphylaxis. The reasons for a tracheotomy not being used are many. It takes a lot of time,is far harder to achieve (getting between the tracheal cartilage is not as easy as it sounds), the risk of “hitting” structures that are vital to the patient are considerable (seen a patient who’s v.jug. ran over the spot) and the required training to do it is considerable - Besides ENTs and sometimes intensivists around here none therefore is even trained to do it anymore. I occasionally teach emergency surgical techniques to interns and med students and we don’t do so,beyond explaining the core concept, neither does any uni in central or northern Europe that I know of, same goes for AU/NZ.
A “cric” is far easier, but still takes some skill - both needle or open surgical cric(I would prefer the later) does require correct identification of the landmarks (which can be tough), good surgical technique and mainly: Training - lots of it. We therefore teach paramedics only a needle based approach (in combination with jet ventilation) - and tbh, most EM docs are not that “up to standard” in this technique as well - even though a cric is far easier than a trach.
The technique mentioned here will, with a 95% chance, not lead to any airway access, damage the thyroid (which bleeds like fuck) or the vagina carotica (the structure that contains the large vessels in the neck as well as the nervus vagus). If that happens the patient is usually beyond rescue. A case that, even if in cardiac arrest, had at least a slim chance of survival, will then certainly die - post anaphylaxis arrests with good bystander CPR have a somewhat improved prognosis - considering that that a laymans trach likely would diminish chest compression quality for minutes this would simply take that chance away from the patient.
Whoever thinks he needs to teach that in civilan responder courses needs to be fired - it’s not part in any curriculum worldwide as they are all more or less based on the same guidelines.